Ovarian Cancer Detection
Scientists are making headway in detecting ovarian cancer at an earlier stage.
(Posted 04/16/10)
In 2009, 21,500 women were diagnosed with ovarian cancer, and 14,600 died of the disease. Though far less common than breast cancer — 192,000 new cases of breast cancer were diagnosed in 2009 and 44,000 people died of the disease — ovarian cancer is almost three times as deadly. Urgent need for early detection
Ovarian cancer is so lethal largely because 75% of cases are diagnosed late, after the cancer has spread beyond the ovaries and often throughout the abdomen. At that point, the five-year survival rate is less than 30%. For the 25% of cases that are diagnosed early, the outlook is very different: a five-year survival rate of more than 90%.
This large difference in early- and late-stage survival makes ovarian cancer an ideal target for improved early detection as an approach to reduce mortality, explains cancer researcher Dr. Steven J. Skates, at Massachusetts General Hospital in Boston. "If we can find it in the early stage, then current therapies are going to cure many women who would have died otherwise." But early detection is difficult for many reasons. Early-stage tumors are only rarely found during a routine pelvic exam, because the ovaries are deep within the body and difficult for a clinician to feel. In addition, ovarian cancer has no known precancerous lesion (unlike colon cancer, which produces a precancerous growth, a polyp, that can be seen and removed during screening with colonoscopy). And while ovarian cancer may produce biomarkers — substances in the blood or urine that indicate something is going on — no biomarker specific to ovarian cancer has yet been identified. CA-125, the biomarker most women have heard about, hasn't worked out so far, though the final results of a large screening trial may change that judgment (see "Ongoing trials" below). Nor do we know whether any of the other biomarkers associated with ovarian cancer and now detected at a late stage are active in the early stages of the disease. Another approach to early detection is transvaginal ultrasound — inserting a transducer into the vagina to obtain ultrasound images of the ovaries. This technique can locate tumors, but most ovarian tumors aren't cancerous, and surgery is the only way to tell the difference. Thus, screening with transvaginal ultrasound alone would result in many unnecessary surgeries for every ovarian cancer found. By contrast, screening for colon cancer and cervical cancer (via colonoscopy and a Pap test, respectively) can identify cancers without major surgery. No test is perfect, so whatever method is used, some women who don't have ovarian cancer will end up having surgeries, Dr. Skates says. "In fact, there's a bar that's been set — and people may be taken aback by this — but the minimum bar for an acceptable screening test is that, at most, 10 surgeries can occur to find one ovarian cancer. Any more than that and the screening approach would be regarded as unacceptable." So far, no single strategy comes close to reaching even this low bar. Where does ovarian cancer start? 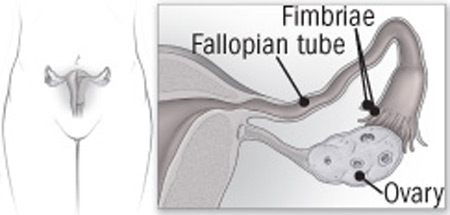 Ovarian cancer has traditionally been thought to start on the surface of the ovary. However, research suggests that some of it arises in the fimbriae, the fringe-like extensions at the ends of the fallopian tubes. What about symptoms? Ovarian cancer has traditionally been called a "silent killer," because symptoms are thought to develop only after the disease has become virtually incurable. But many women who've had the disease disagree, reporting they had distinctive abdominal pain or digestive problems well before they were diagnosed. In a 2007 study, researchers at the University of Washington led by Dr. Barbara Goff identified a set of physical complaints that often occur in women who have ovarian cancer. This "symptom index" formed the basis of a consensus statement released later that year outlining four symptoms that may be early warning signs: bloating or distension of the abdomen, pelvic pressure or pain, difficulty eating or feeling full quickly, and the need to urinate often or urgently.
Some experts remain skeptical; they think early-stage ovarian cancer doesn't produce these or any other symptoms, and that the symptom index serves only to identify treatment-resistant late-stage cancers. Others worry that these symptoms are too vague and accompany too many other health problems, such as irritable bowel syndrome, menstrual difficulties, and bladder infections. One study found that for every 100 women in the general population who experienced them, only one would actually have early-stage disease. Nevertheless, many specialists agree that they're the best we can do for now, and that women with new, unexplained pelvic symptoms that persist for a month should see their clinicians. Ongoing trials Two large, controlled trials are under way to find out if ovarian cancer screening with CA-125 plus vaginal ultrasound improves survival rates among postmenopausal women at average risk for the disease. Preliminary findings were reported in 2009, but final results, including mortality data, aren't expected for several years. As part of the National Cancer Institute's Prostate, Lung, Colon and Ovarian Cancer Screening Trial, more than 75,000 healthy women were randomly assigned to undergo either usual care or annual CA-125 testing plus transvaginal ultrasound. If a woman's CA-125 or ultrasound test was positive, she was referred to a gynecologist for follow-up. The results so far have been disappointing. After annual screening for more than four years, 19.5 women on average had undergone surgery for each identified case of ovarian cancer — far from the aforementioned "bar" of no more than 10 surgeries to detect one ovarian cancer — and 72% of the cancers detected were already at a late stage. The preliminary findings have been more promising in the United Kingdom Collaborative Trial of Ovarian Cancer Screening, which Dr. Skates helped design. More than 202,000 women at average risk for ovarian cancer were randomly assigned either to no screening, annual transvaginal ultrasound alone (with repeat ultrasounds and clinical evaluation as needed), or a "multimodal" approach consisting of annual CA-125 testing followed by transvaginal ultrasound for selected subjects based on their CA-125 results. In the multimodal group, if a woman's CA-125 began to rise significantly above her baseline level, an accelerated schedule of CA-125 testing or ultrasound kicked in, based on a special ovarian cancer algorithm, or set of rules. Results from the first year of screening showed that nearly 50% of cancers detected in both screening arms were early-stage — a doubling over usual care, where 25% are found at an early stage. The average number of surgeries needed to find one cancer in the CA-125 plus transvaginal ultrasound group was an impressive 2.9; in the ultrasound-alone group, on the other hand, 35.2 surgeries were required to find one cancer. While these first-year findings are encouraging, the final results of subsequent years of screening are the most important indicator of the long-term impact of this screening approach. Until those results are reported, no definite conclusions can be made. The United Kingdom trial is scheduled to end in 2015. Although CA-125 is still generally considered a late-stage marker, Dr. Skates thinks it might serve as an early indicator in women at average risk as long as the testing is personalized. That would mean carefully tracking CA-125 values over time and evaluating fluctuations in relation to a woman's individual background level. Why CA-125 alone isn't a good screening test
Many women ask to be screened for ovarian cancer with a CA-125 test. While a CA-125 reading can be a helpful tool, it doesn't qualify as a good screening test, and here's why:
A screening test is a test that's done in a person with no symptoms in order to find disease early enough for successful treatment. A good screening test should be highly sensitive, meaning that it gives a positive result when the illness is present. In this case, a test that's 100% sensitive would detect all cases of ovarian cancer. It should also be very specific; that is, the results are negative when there's no cancer. CA-125 is a protein often made by ovarian cancer that circulates in the blood. Levels of CA-125 are elevated in about 80% of women with advanced ovarian cancer but only 50% of those with early-stage disease. Thus, CA-125 isn't sensitive enough: it could miss as many as half of all women with early-stage cancer. It's not specific enough, either, because it's elevated by many other conditions, including other cancers, endometriosis, fibroids, and pelvic infections. Specificity is extremely important because only one in 2,500 women develops ovarian cancer every year. To understand the problem, imagine screening a representative group of 2,500 women, and suppose our test is 100% sensitive (it identifies every woman with the disease). Now suppose the specificity is 99%, meaning that 1% of the women test will positive even though they don't have ovarian cancer. In screening our group of 2,500 women, we would find one case of ovarian cancer, but we'd also get false positive results for 25 women. Unfortunately, invasive surgery is the only way to find out for sure which is which. Consequently, to locate the one woman in 2,500 who actually had the disease, we'd have to subject 25 others to unnecessary abdominal surgery. Now expand the screening group to include all U.S. women; the number of unnecessary surgeries would be huge. Thus, the risk of general screening with CA-125 alone far outweighs the benefit. New developments
It's long been thought that most ovarian cancer starts on the ovary's surface (epithelium), but research by pathologists at Harvard's Brigham and Women's Hospital in Boston and elsewhere is changing that picture. It now appears that some ovarian cancer arises at the end of the fallopian tubes, in the fimbriae, the finger-like projections that brush the ovary (see the illustration). This discovery has led some scientists to speculate that early-stage and late-stage ovarian cancer are actually two distinct diseases.
Dr. Michael J. Birrer, director of gynecologic medical oncology at Massachusetts General Hospital, believes fimbrial-end ovarian cancer may account for the 75% of cases that turn deadly: "It's because it's sitting out there in the open, sort of flapping around, that those cells break off and latch on to the ovary, and more importantly, spread throughout the abdomen very early in their natural history. That's versus the ‘good' ovarian cancer, which we think may come from...cysts within the ovary." Those cancers, he says, "probably evolve into the tumors that have a longer latency period and can be felt by pelvic exam and removed surgically." Not everyone agrees that fimbrial-end tumors play such a large role, but if it turns out that some ovarian tumors are more aggressive than others for genetic reasons, then genomic techniques may help identify targets for new therapies. Dr. Birrer, Dr. Skates, and other scientists are also using advanced technologies such as mass spectrometry to look for more precise biomarkers of the disease.
What now? Although research is proceeding apace, the findings haven't matched the progress that's been made, for example, in breast cancer research and treatment. But there are certain steps you can take: Know your risk. CA-125 and transvaginal ultrasound can be of use in women at high risk for ovarian cancer. You're at high risk genetically if you have a mother, sister, daughter, grandmother, aunt, or niece who had the disease. Carriers of the BRCA1 or BRCA2 gene mutations are also at increased risk. Most experts recommend combination screening of high-risk women with CA-125 and transvaginal ultrasound every six months. Among such women, a positive CA-125 test is more likely to be a true positive, so the risk of invasive surgery may be worth taking. High-risk women who are past childbearing may also want to consider having their ovaries removed — a procedure that's 90% effective in preventing ovarian cancer. Pay attention to abdominal symptoms. If you're at average risk for ovarian cancer, pay attention to new abdominal or pelvic symptoms that persist for a month or more even when you've tried such strategies as laxatives, exercise, and diet change. You know what's normal for you, so if you're concerned, see your gynecologist for a thorough pelvic exam. If the pelvic exam raises suspicions, it should be followed up with transvaginal ultrasound and possibly a CA-125 test. If you need surgery, it should be performed by a gynecologic oncologist or other surgeon skilled in ovarian cancer treatment. Reprinted with permission from Harvard Womens Health Watch

Top of Page
Back to Women's Health Information
| 



 Home
Home
 What's New
What's New Professional Advice
Professional Advice


